Hair loss meds have an “offense” and “defense”
I went digging into hair-loss meds. The simple split: regrow (minoxidil) vs keep (finasteride/dutasteride). This is a personal summary of the 2017 Japanese Dermatological Association guideline. Not medical advice—talk to your doctor.
https://www.dermatol.or.jp/dermatol/wp-content/uploads/xoops/files/AGA_GL2017.pdf
(As of 2025 this 2017 edition is still the latest.)
The guideline in a nutshell
It’s compiled by dermatology professors and clinicians in Japan. It ranks treatments from “strongly recommended” to “should not do,” based on clinical evidence over months to years.
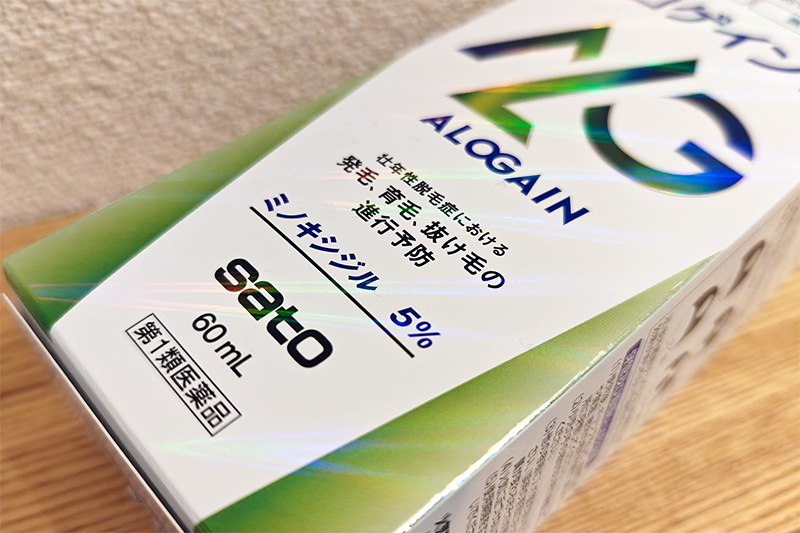
Offense: topical minoxidil (5%) — strongly recommended (Grade A)
Originally a blood-pressure pill (Loniten); patients grew hair as a side effect, so the topical version became a hair-loss drug.
Evidence example: a 48-week RCT with 393 men showed non-vellus hairs per cm² increased by ~3.9 (placebo), ~12.7 (2%), and ~18.6 (5%); 5% beat the others significantly.
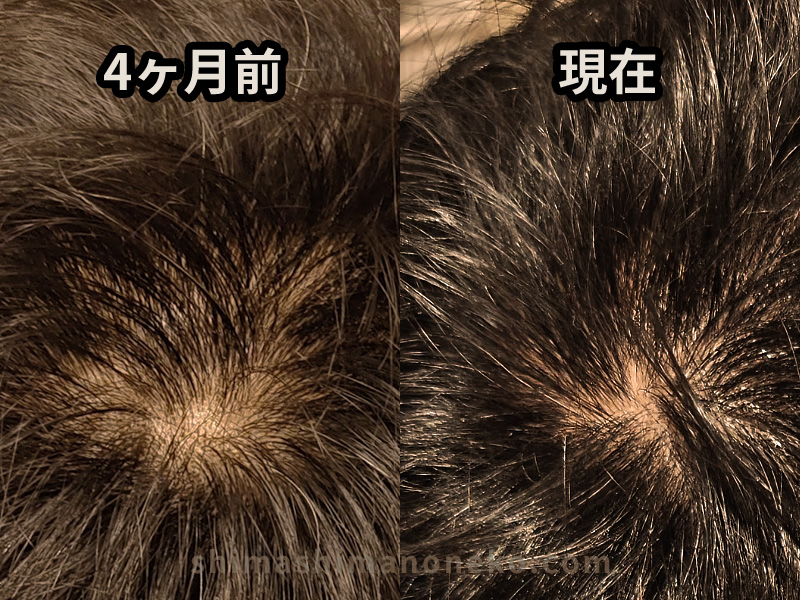
In short: 11 months of 5% topical grew hair, with photos to prove it.
 Source: Hair loss Q&A (JDA)
Source: Hair loss Q&A (JDA)
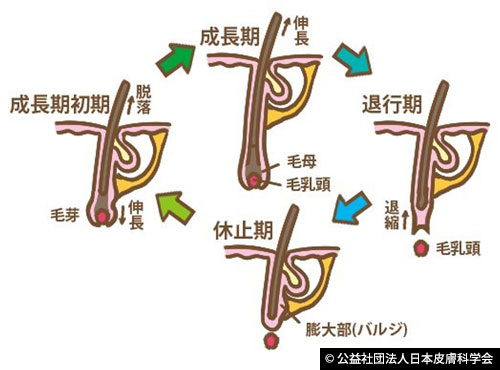
Why “offense”? It reactivates resting follicles. When a resting hair restarts, the weak hair sheds once and a new anagen hair grows—this is why early shedding happens.
Early shedding can occur; warn patients so they don’t quit.
Side notes
Redness or itch can happen. If it burns, swells, or worsens, stop and see a dermatologist.
Defense: finasteride / dutasteride — strongly recommended (Grade A)
DHT (a potent androgen) shortens the growth phase and tells scalp hair to “take a break,” while it feeds beard growth. These drugs reduce DHT production, so less “take a break” signals reach scalp follicles. Think of it as removing the saboteur rather than forcing growth.
In a 5-year observation of 801 Japanese men on finasteride 1 mg/day, photo evaluation improved in 99.4% of cases; younger and milder cases did even better.
A 6-month observation (27 men) showed Quality of Life scores improving (VAS and DLQI).
Overall: about half to one year for noticeable regrowth; multi-year use improves survival of existing hairs.
Side notes
- Acts on male hormones; contraindicated in pregnancy due to fetal risk.
- PSA (prostate cancer screening) values drop about half; tell your doctor before blood tests.
Finasteride is branded “Propecia”; dutasteride is “Zagallo” in Japan. Efficacy is similar; dutasteride is newer.
Support: adenosine — recommended (Grade B)
Supports hair-matrix cell growth and extends growth phase; boosts blood flow a bit (less than minoxidil). A 0.75% lotion showed similar usefulness to 5% minoxidil lotion in one study. It doesn’t “restart” dormant follicles, so it’s supportive, not a core regrowth engine.
Support: carpronium chloride — optional (Grade C1)
Known as “Karoyan” in Japan. A blood-flow enhancer with mild growth effects; long history, low downside. Also used adjunctively for alopecia areata and vitiligo.
Poor risk/return: oral minoxidil — should not do (Grade D)
Grade D = “should not perform; evidence of ineffectiveness or harm.” Oral minoxidil is still a blood-pressure drug; hair growth is just one side effect. Other side effects cluster around heart and circulation:
- Swelling, water weight gain
- Faster heart rate, palpitations
- Shortness of breath, chest pain
- Congestive heart failure, pericarditis
Low doses can seem “fine” for some, but risks depend on age, blood pressure, conditions, and other meds. Because cardio effects can be silent, routine use isn’t advised.
Why Grade D?
- No country has approved it for hair loss
- Long-term safety data are lacking
- Cardiovascular side effects occur in a nontrivial share
It’s more “not enough to responsibly recommend” than “instantly lethal,” but absent approvals or robust long-term data, it stays off-guideline.
Poor fit for root-cause treatment
Thinning stems from DHT-shortened cycles; simply forcing follicles to grow while DHT keeps attacking is like planting seeds into pest-ridden soil. Without blocking DHT, oral minoxidil alone isn’t addressing the root cause.
Wrap-up
Hair-loss meds aren’t a simple power ranking; they’re roles: offense (minoxidil), defense (finasteride/dutasteride), and support (adenosine/carpronium). Modern options wake resting follicles or block hormonal triggers, while older blood-flow boosters linger as mild, low-risk helpers.
Topical 5% minoxidil plus finasteride/dutasteride already has strong evidence; that’s the safest, most proven starting point.
I recovered with topical minoxidil. Details of my four-month experience here:

If you want to judge your crown more confidently, see: